The ISO 10993-1 biocompatibility matrix now serves as a tool for determining which information requirements to use. Chemical analysis is now available in all categories. This does not always necessitate testing, but it does necessitate knowledge of potential toxicity.
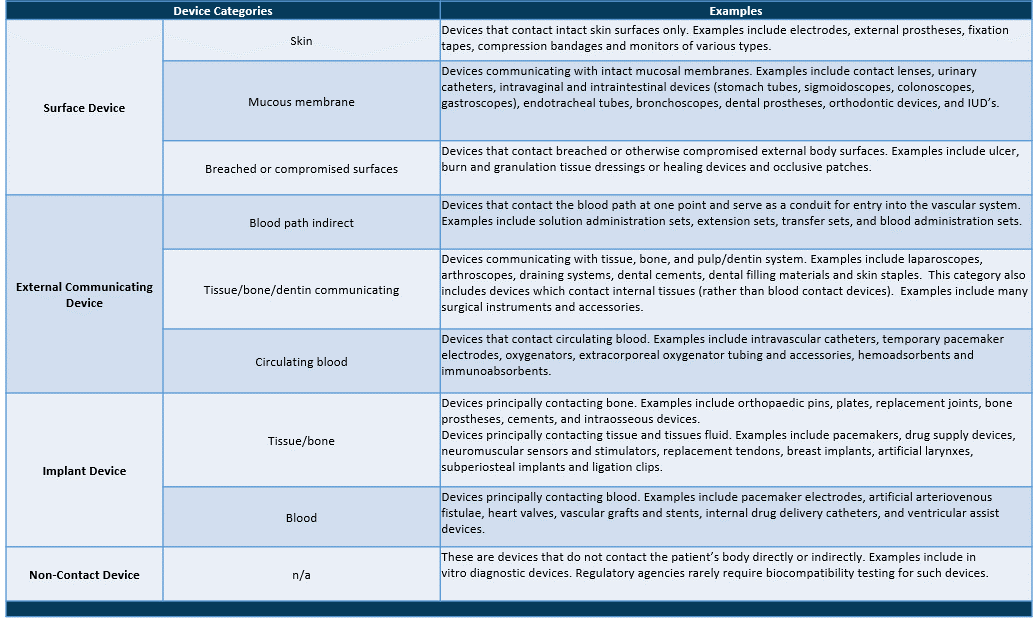
Device Categories – Definitions & Examples
When using the biocompatibility matrix philosophy, it is clear that the rigor of chemical analysis and any associated toxicological risk analysis can be tailored to the device’s application.
As a result, continuous skin contact would necessitate less intensive extraction and investigation of chemical migrants. A long-term implant, on the other hand, would necessitate extensive extraction and analysis, as well as a thorough risk assessment of all materials identified.

Following the preceding analysis, it is logical to assign different levels of analysis to meet the biocompatibility matrix’s requirements. (The analytical methods are briefly described at the end of this document.)
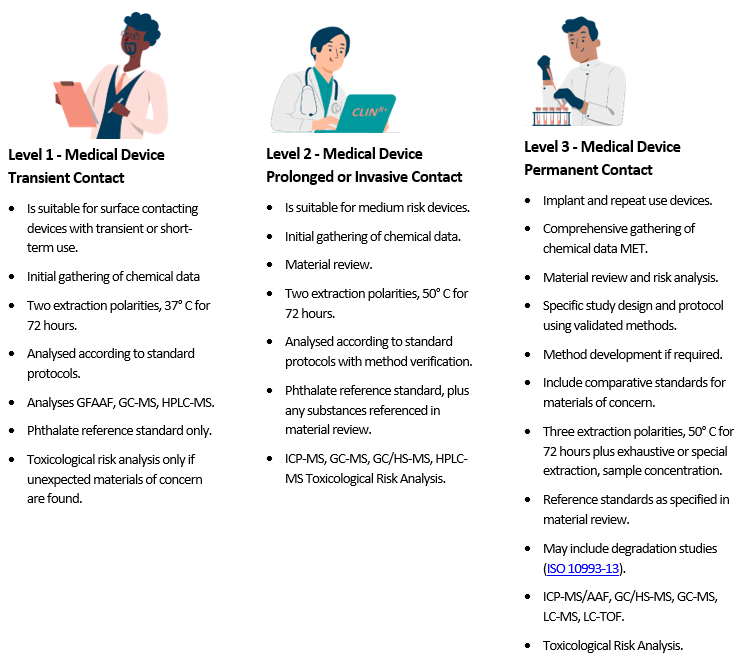
Table 1 – Standard surface areas and extract liquid volumes

Table 2 – Standard extraction conditions

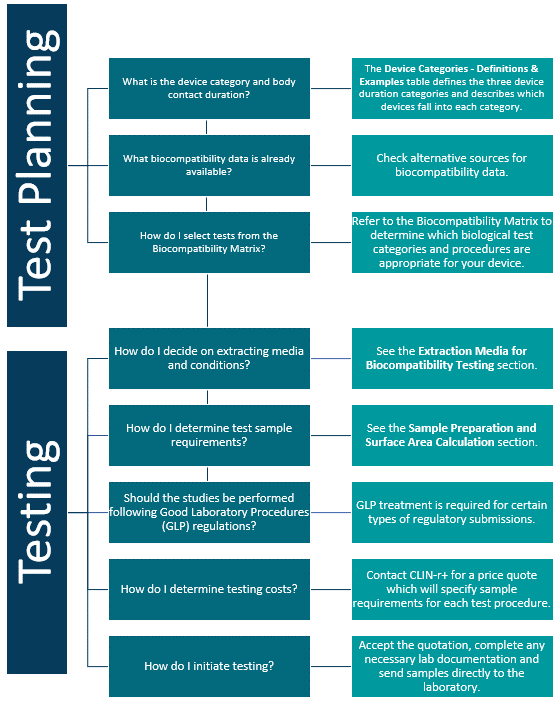
Device companies spend a tremendous amount of time, money and energy developing and implementing biocompatibility testing programs. Below is a Biocompatibility Planning Tool to guide you through the basic concepts of device testing and to help manufacturers select testing procedures to comply with current regulatory requirements.
The chart below gives you an overview of the process. The potential toxicity of the materials, both individually and in combination, is then quantified using a variety of data sources.
Medical device biocompatibility problems are most often caused by toxins that leach out of the device into the surrounding tissues or body fluids. So, in the laboratory, extracts of device materials are often used in assessing biocompatibility. These extracts are generally prepared using exaggerated conditions of time and temperature to allow a margin of safety over normal physiological conditions.
Analytical extraction studies allow the chemist to identify and quantitate specific leachable moieties. This data can in turn help the device toxicologist or risk assessor determine the worst case scenario for patient exposure and the risk to patient health.
Extracts are also used in many of the biological tests specified by ISO 10993.
Table 1 below lists the most commonly used extracting media. For most devices, only saline and vegetable oil extracts are needed.
Extracts are selected on the basis of the biological environment in which the test material is to be used. A saline (SCI) extract approximates the aqueous, hydrophilic fluids in the body. It also permits the use of extreme temperatures in preparing the extracts, thus simulating certain sterilization conditions.
Tissue culture media may even more closely approximate aqueous body fluids but cannot be used for high temperature extractions. Vegetable oils are non-polar, hydrophobic solvents and simulate the lipid fluids in the body. For technical reasons, DMSO extracts are often used in certain genotoxicity and sensitization tests. Two other common extracting media – Alcohol in SCI and PEG – should be used only if they approximate the solvent properties of drugs or other materials that will contact the device during its normal use.
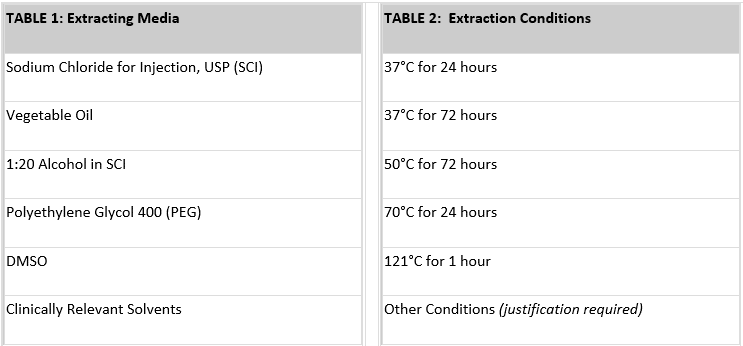
Extraction conditions (temperature and time) should be at least as extreme as any conditions the device or material will encounter during sterilization or clinical use. Generally, you will want to choose the highest extraction temperature that does not melt or fuse the material or cause chemical changes. To provide some margin of safety for use conditions, Pacific BioLabs recommends an extraction condition of at least 50°C for 72 hours. For devices that are susceptible to heat, an extraction condition of 37°C for 72 hours may be acceptable. Table 2 above lists common extraction conditions.
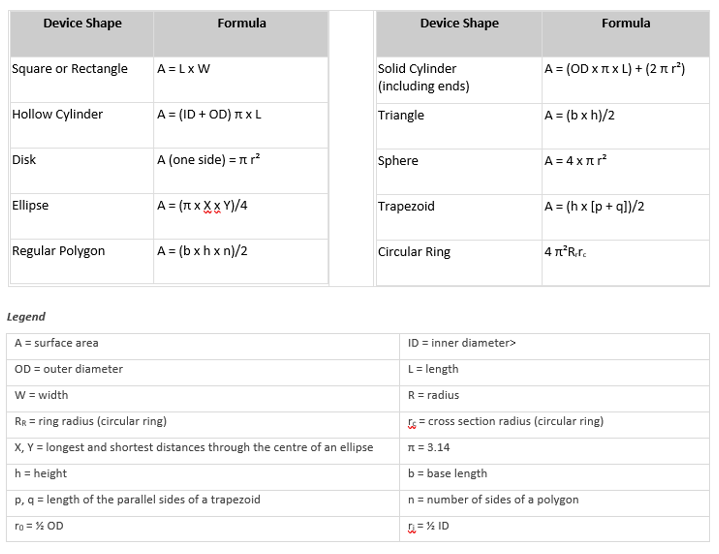
The simplest method for determining the surface area of a device is usually to use the CAD program from the design engineering group. Typically, the surface area can be calculated with just a few keystrokes. Alternatively, you can calculate the surface area using the equations below. Or you can submit a sample device and/or an engineering drawing to CLIN-r+, and our staff will perform the calculations.
Typically, the standard surface area of your device is used to determine the volume of extract needed for each test performed. This area includes the combined area of both sides of the device but excludes indeterminate surface irregularities. If the surface area cannot be determined due to the configuration of the device, a mass/volume of extracting fluid can be used. In either case, the device is cut into small pieces before extraction to enhance exposure to the extracting media. In some cases, it is not appropriate to cut the device; such devices are tested intact.
The Test Turnaround Time and Sample Requirements table lists the amount of sample required for many procedures. Generally, we recommend using the ratio of sample to extracting media specified in ISO 19993-12 (i.e. either 6 cm²/mL or 3 cm²/mL, depending on the thickness of the test material). For some types of materials, the ratio used for USP Elastomeric Closures for Injections (1.25 cm² per mL) is preferred.
Formulas for Surface Area Calculation